

Can anything be salvaged from the genocide of tens of millions from C19 injections?

Let’s start with a few questions.
Why would you not develop an anti-toxin to the toxic spike protein, rather than inject the toxin itself? Anti-toxins/anti-venoms are cultured in animals FIRST and injected into snake-bite victims on a per bite basis – NOT into an entire population that might get bitten by a snake.
Why would you START an injection roll-out in those with weakened immune systems from age and infirmity? The elderly and infirm already have weakened immune systems and yet the theory is that this weakened immune system can somehow mount an immune response to a toxin from that weakened immune system?
No doubt toxicologists and virologists have the answers at their fingertips to these questions.
Ok, assuming there are easy and available answers to those questions that I have missed because of my (lay-person’s) ignorance, let’s press on to salvaging something from the wreckage of genocide of tens of millions.
I started this train of thought with the articles below about the Russian viral vector injection, Sputnik V, its ties with the Oxford/AstraZeneca viral vector injection and the withdrawal of the Oxfor/AstraZeneca injection from all over the world, except India (where 80% of the country has been injected with it and where adverse event data is woefully inadequate – as reported by the BMJ back in January 2022 here:
How covid-19 vaccines exposed India’s adverse events reporting system | The BMJ
Here are some links to the Sputnik V – Oxford/AstraZeneca “story”.
(100) Russians are also "dying suddenly" - Edward Slavsquat (substack.com)
(100) Sputnik V: It's what "alt media" craves! (substack.com)
The Russian C19 viral vector injection has close ties with the Oxford/Astra Zeneca viral vector injection, on a “stand-alone” basis and as a “mix and match”. It looks as if the “technology” was transferred to Russia and rolled out in August 2020 – four months before the mRNA and viral vector injections elsewhere in the world.
Is the Sputnik V vaccine too good to be true? We need the data - STAT (statnews.com)
It is hard to leave aside the potential for a rate for the Oxford/AstraZeneca “kill-shot” of possibly five times the 1 per thousand “kill shot” rate of C19 mRNA injections for 80% of 2.2 billion shots into Indian arms
80% of doses administered in India were the Oxford/AstraZeneca kill shots licensed to the Serum Institute – 2.2 billion times 80% times 5 per thousand killed = 8.8 million dead over the last two years. There are 1.4 billion people in India – maybe they don’t even notice an extra 80,000 deaths a week for two years. Maybe the death toll is not so high because there is/was widespread use of Ivermectin that negated the impact of the kill shots. I doubt anyone in India is even investigating.
Back on track. What can be salvaged from the wreckage or is the entire mRNA and viral vector technology simply a complete and utter failure. Lord knows the technology is in our meat, poultry and dairy products now and similar technology has been in crops in the form of GMO crops for decades.
Here’s the “deal”.
We have to rigorously examine Phase IV of the clinical trial process – even though we know the first three phases were “warped” and fraudulently conducted or omitted entirely.
From here, there is a description of each phase of the clinical trial process - a process which normally takes ten to 15 years!
What is a Phase 4 Clinical Trial? (news-medical.net)
“Prior to the phase 4 trial
In phase 1 clinical trials, the safety, tolerability and toxicity of the drug at different doses is tested in a small number of healthy volunteers. In phase 2, the drug's efficacy and optimal dosing regimen are established.
After phase 2, the drug enters the most vital stage of its development, the phase 3 trial. This is the last phase of testing the drug needs to complete before the drug information and clinical trial results are submitted to the regulatory authorities for approval of the drug for use in the general population.
Phase 4 trial
The phase 4 trial is also referred to as post marketing surveillance and as the name suggests, it is conducted after the drug is already marketed and available to the general public. The main objective of the phase 4 trial is to check the drug's performance in real life scenarios, to study the long-term risks and benefits of using the drug and to discover any rare side effects.
In a phase 4 trial, any rare or long-term effects of the drug can be observed in a much larger population of patients and over a much longer period of time. If safety surveillance does indeed reveal concerns about the drug, it may be withdrawn from the market and no longer made available on prescription.”
There are two geographies for which Phase IV (not a trial really – an observational analysis) can help salvage something from the wreckage. Argentina and the EU.
A rigorous, unbiased and detailed analysis of a host of injections and a placebo should be readily available.
I suggest that 5,000 people who received each of the many different C19 injections rolled out across the world plus a 5,000 placebo group in each of the EU and Argentina would be sufficient to yield statistically significant results for deaths and adverse events of the many different injections. Others might consider 10,000 to be a minimum.
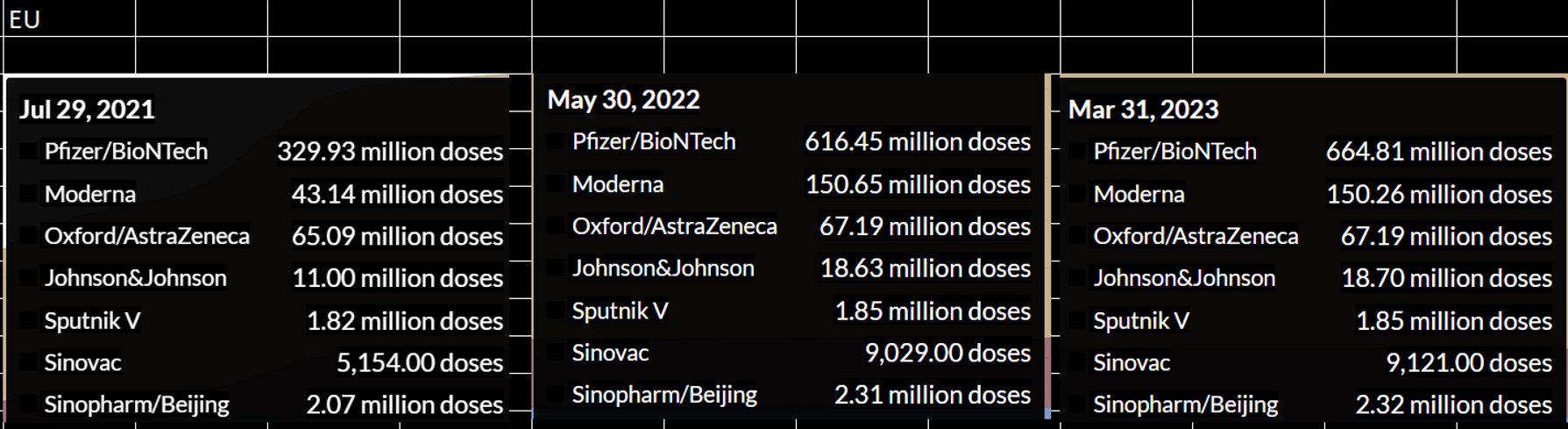
Here is some data on the different injections by manufacturer in each of EU and Argentina.
I have selected ten month gaps for ease of reference.

If such a thing as a world health organisation existed, it would be something that would fall within its remit. Perhaps the WHO can, finally, pretend to be such a thing There are 8,500 people working for the WHO and it says we are in a public health emergency of international concern.
Maybe it would not be necessary to get study data for Pfizer/BioNTech and Moderna in Argentina or Oxford/AstraZeneca, Sputnik V and SinoPharm in the EU.
A study of this sort should not take more than a few months.
In a sane world, governments around the world would leap at the chance to fund this sort of study and would claw back the odd 100 million bucks it would cost – with a 1,000 dollar incentive for 80,000 study participants to provide their time and medical records, plus record checking for deaths.
No doubt though, we are living in a Clown World where evidence, science, medicine and the truth are the enemy of the people, rather than their salvation.
We all learn by mistakes. What we have currently is “clinical trial and genocidal error”. The entire mRNA platform needs to be stopped until it is safe, right now it is clearly UNSAFE and has already caused one global holocaust with several more in the offing.
In a sane world, ALL vaccines would be re-trialled to test for corruption of captured regulatory bodies.
Onwards!
Please upgrade to paid, or donate a coffee (I drink a lot of coffee) - “God Bless You!” if you can’t or don’t want to contribute. Coffee donations here: https://ko-fi.com/peterhalligan
Unless people of all political types who were involved with these deadly decisions are truly held liable for this inhumanity then THEY and their cartels will do the same or worst given the next planned event. Death...and the loss of loved ones... has been so cheapened by these diabolical people...but they do not care...this is a war to them...remember they wanted to jail all who had a different opinion about climate change.
"No doubt toxicologists and virologists have the answers at their fingertips to these questions."
Ehh, no they don't. Absolutely not. Sarc tag omitted?
A lot of hand waving and confabulation, but no answer where there is none, notably when the shots demonstrate profoundly unpredictable, negative risk benefit, or a notional NNV of 217 (ARR of 0.46%), and a list of adverse consequences that read like a compendium of clinical pathology, up to and including the millions upon millions of relatively immediate deaths to which you allude.