

Effectiveness (not safety) of slower changing C19 “vaccines” is different against faster changing variants - from 90% for “wild” initial variant to negative for latest KP variant
A Quebec study discussed by Professor Clancy and Dr Campbell

From here, a Quebec study covering the period from 2021-2024, shows that the changing “vaxx” was not matched to circulating variants:
Data on COVID-19 in Québec | Gouvernement du Québec
With a link to this:
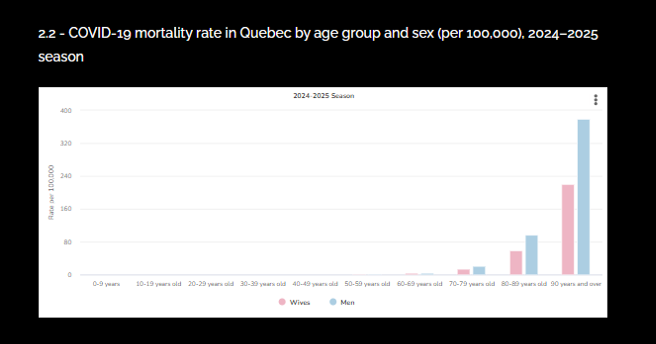
COVID-19 data by period by age and sex in Quebec | Institut national de santé publique du Québec
“The most recent data on the evolution of COVID-19, for the week of February 16 to 22, 2025, in Québec show:
737 new cases cases for a total of 1,523,952 cases
14 new deaths for a total of 21,221 deaths “
“Sources:
The data source for COVID-19 deaths has changed. This change was applied throughout the pandemic period. Considering that the new source only provides deaths in the underlying cause (direct death from COVID-19), a decrease in the number of cumulative deaths is observed.
Matching data on emergency room visits from the Système d’informationet de gestion des urgences (SIGDU), hospitalizations (regular and preliminary) from MED-ECHO, and positive PCR laboratory tests for SARS-CoV-2, as of February 27, 2025 at 11 am. The hospital centers selected are the general and specialized hospital centers offering mainly acute care.”
Quebec has a population of 8.5 million.
Which has charts like this:
Professor Clancy discusses the report here:
Zero vaccine efficacy predictable
The experimental modified, C19 mRNA injections were 90% effective against the first “wild” variant and the BA1’s and 2’s - but waned over time against emerging Omicron variants.
Vaxx contained ingredients against XBB 1.5 - but the virus had moved on.
JN1 variant was prevalent - vaxx effectiveness dropped to 50%.
KP variant, VAXX EFFECTIVENESS WAS ZERO TO NEGATIVE.
This reflects the changing population, the vaccine contents and the shift (not a slide) in the circulating variants, The virus “shifted” it did not “drift”.
Uncontrolled antigen being presented everywhere.
The other DNA C19 “vaccine” is more focussed on the source of the disease, than the experimental modified mRNA C19 “vaccine”.
Here’s the first part of the write up on YouTube:
“Link to Quadrant, https://quadrant.org.au/news-opinions...
Monovalent mRNA XBB.1.5 vaccine effectiveness against COVID-19 hospitalization in Quebec, Canada: impact of variant replacement and waning protection during 10-month follow-up https://www.medrxiv.org/content/10.11... Protection Conferred by COVID-19 Vaccination,
Prior SARS-CoV-2 Infection, or Hybrid Immunity Against Omicron-Associated Severe Outcomes Among Community-Dwelling Adults https://academic.oup.com/cid/article/...
Comparing frequency of booster vaccination to prevent severe COVID-19 by risk group in the United States https://www.nature.com/articles/s4146...
Two-Dose Severe Acute Respiratory Syndrome Coronavirus 2 Vaccine Effectiveness With Mixed Schedules and Extended Dosing Intervals: Test-Negative Design Studies From British Columbia and Quebec, Canada https://academic.oup.com/cid/article/...
COVID-19 mRNA VACCINES: THE PROBLEM THAT WON’T GO AWAY. Emeritus Professor Robert Clancy AM
This month we ‘celebrate’ 5 years since the covid pandemic began in Australia. This is the 10th article I have written for Quadrant on covid pandemic management. Prior to the pandemic my 300+ publications had been in peer reviewed medical journals.
Most reported research on airway immune protection which has been my passion for 50 years. In 2019 the University of Newcastle awarded me a Doctor of Science for this work (I was informed that this was the first such award given by the University).
My point is that in 2020 with the appearance of SARS-CoV-2 (the virus causing Covid-19), entirely by circumstance, I was as well placed as anyone to understand this new airway infection, its pathogenesis and its management. Specifically, the likely place for vaccination in the control of the pandemic. That is what I did.”
The analysis does not address the safety of the “vaccines”. Once these are reflected, the latest version of the “vaccines” becomes “all harm ad no benefit”.
Which rather begs the question - “why not develop “vaccines” that target the variants and chase them down - ad infinitum - if medics thought that this was appropriate for the first variants?”.
The answer is, of course, “it was never advisable to do this, since this forces new variants”!!!
Thiis was known at the outset in 2020, five years ago. Al that fuss, money and harm - for a know outcome of forcing new variants,
Please take a paid subscription to reward me for the thousands of hours of research that go into the thousands of SubStack articles I publish - or make a donation of $3 bucks or more for a ko-fi here:
Onwards!!!
Go on www.nextstrain.org and follow SARS-CoV-2. You will quickly realize that it became obvious within months of identifying COVID that the idiots recommending vaccinations ad nauseam were merely chasing their tails. There are probably over 6,000 variants of the original COVID by now and by the time someone pretends they know which strain to target with yet another pseudo-vaccine, another 300 have come into the equation.
This was obvious from the beginning, virologist Dr Geert vanden Bossche pointed out that because these are not sterile vaccines, this Immune Pressure will continue to produce more and more variants, and may actually eventually lead to one that is more deadly.
The idiots still pushing COVID shots no doubt own stock in pharmaceutical companies, as it has been obvious since there are nine pages of Adverse Events for just the Pfizer “vaccine”, that the good cannot outweigh the bad with COVID shots, especially using the mRNA platform.
What do you make of this?
https://pubmed.ncbi.nlm.nih.gov/39903865/