If only HCQ and IVM protocols had been used instead of "vaccines"
1.6 million lives and almost all C19 deaths and injuries

US C19 injections cause one death per thousand doses (up 27% in 2022) with 6% causing an “adverse event”
WTF is going on? Incompetence, Corruption or Malice, or all three?
My previous two posts set out the data used by the CDC to characterize the impact of the COVID-19 (C19) pandemic on mortality numbers.
There are many errors, mischaracterizations, and omissions in the data. Notably, for example, excluding 116,000 drug deaths in 2020 and 142,000 in 2021 that place drug deaths as the 6th leading cause of death behind “Strokes”.
Enquiring minds want to know why the US CDC/FDA recommends C19 injections for children when the data shows that C19 poses no risk and developed countries in the EU and in the UK have withdrawn them. What metrics is the CDC/FDA ignoring? To me the injection of children is an ABOMINATION. The crude mortality rate for umder 14-year-olds, using the CDC’s own data, is constant over the entire pandemic and is equal to the crude mortality rate in prior years.
We are seeing increasing proof of pre- and post-natal harms PLUS male and female fertility issues. We know the injections penetrate cells. No-one is yet talking about hereditary issues for descendants of the injected. Maybe there is another trial with 8 white mice underway that we are not aware of.
I am curious to know what the “stopping condition” is for the WHO to withdraw its Public Health Emergency of International Concern ()PHEIC, pronounced FAKE). After almost three years, the pandemic is characterized by a 2.8% annualized case rate wth a 97% recovery rate after a 15 day infection. For the US, these numbers are a much higher 10.7% annualized case rate, but the same 97% recovery rate. I am also curious as to why the recovery rate is not even calculated within clinical trials to show the relevance of the disease itself.
In the same way that “cases” were never split between “asymptomatic” and “symptomatic” using the RT-PCR test, the manner in which 97% of cases “recovered” is not known – neither is the incidence of previous C19 infections amongst deaths and casualties within VAERS. For all we know, getting injected on top of a prior infection heightens mortality and morbidity risk – likewise, maybe treatment protocols, including IVM and HCQ, are coincident to recovery, not causal. If the average recovery period is 15 days for the majority of people (say, 90% out of 97%) why is any treatment necessary at all amongst the healthy, so (as per FCCC recommendations) only that fraction of people with 2-6 co-morbidities that are 1-2 years older than life expectancy should even be considered for any treatment protocol.
The recent release of V-Safe data for 10 million cell-phone contributors confirmed the 25% adverse event rate from injections that was revealed in Pfizer’s clinical trials. Of course, a death is not going to be reported to V-Safe.
Okay, let’s dive in with a snapshot of the pandemic so far. Keep in mind that “cases” and “deaths” are diagnosed using the (Christian Drosten) RT-PCR test that has (falsely) been used to determine the presence of the SARS-COV2 virus that causes the CoVID-19 disease.
Christian Drosten & the Fraud Behind COVID 19 PCR Testing | Principia Scientific Intl. (principia-scientific.com)
https://principia-scientific.com/christian-drosten-the-fraud-behind-covid-19-pcr-testing/
This test was withdrawn from Emergency Use Authorization on 31 December 2021 because it could not distinguish between different flu viruses and their variants. Deaths are shown with C19 “present” and are not necessarily the cause of death. Keep in mind that injection deaths and injuries that occur within 14 days of injection are “thrown” into the “unvaccinated” bucket and ascribed to another non-C19 condition or death. - but C19 “cases” and “deaths” with C19 “present” are calculated within 60 days of a “positive” RT-PCR test.
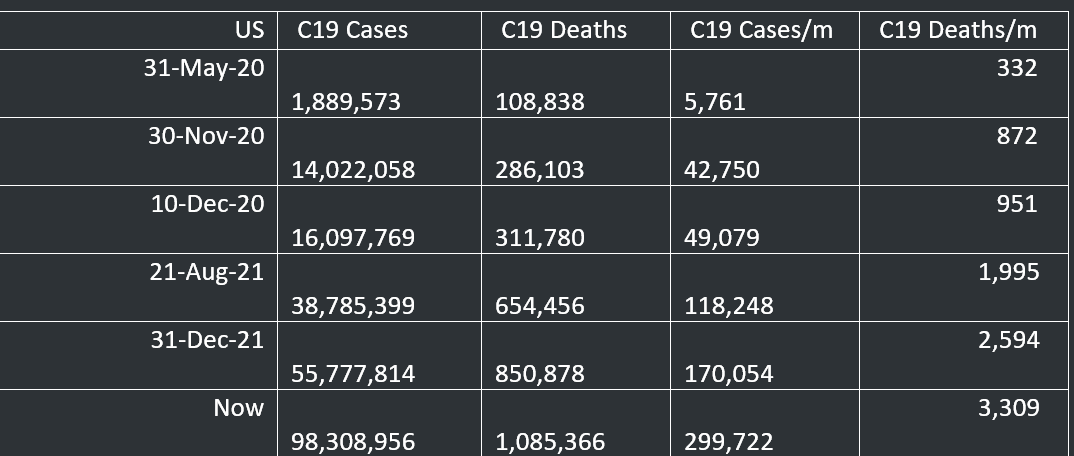
The “broken” dates have been chosen as follows:
· 31 May 2020, start of Pfizer clinical trial – 30 November 2020, end of that trial.
· 10 December 2020, launch of injections
· 21 August 2021 – publication of Dr. Jessica Rose’s paper calculating a URF of 41
Let’s leave aside a possible adjustment to the number of C19 cases and deaths to reflect the false positive results from not calibrating the RT-PCR test to the actual isolated virus and the use of 35-40 amplification cycles when any cycle use over 24 results in as many as 95% false positives (or that the inventor of the RT-PCR test, Kary Mullis, stated that it could not be used to diagnose infectiousness).
This is the base case, before alternative treatment protocols that should have been rolled out and which woujld have prevented the roll-out of injections.
Started at the two minute mark here for “the forcing” - the whole video 6:28 minute is worth watching.
Rise of the VARIANTS - YouTube
https://www.youtube.com/watch?v=5a7PLv9JkF4&t=120s
What would have been the path of the pandemic had alternative treatment protools like IVM and HCQ been used instead. Dr Zelenko’s protocol of HCQ+Zn+Azm was known well before the clinical trials even started In May 2020. Trump and Atlas were all for the HCQ protocols. The corrupted FDA/CDC/NIH/NIAID/WHO complex was not. The MSM was complicit in ridiculing HCQ protocols – remember the wife who tried to murder her husband with fish tank cleaner that had a similar name? The MSM could not push the false narrative that HCQ was unsafe fast or hard enough.
Similarly, treatment with IVM was known to work by the start of the mRNA “vaccine” clinical trails in May 2020. A year later, IVM’s effectiveness was demonstrated in Uttar Pradesh state of India, where it obliterated C19 entirely. The states’ population of 240 million achieved zero CoVID19 – with the administrative assistance of the WHO, on the ground in the state. The FDA response? “You are not a horse, you are not a cow. Seriously, y’all, stop it”. There will be a siigle employee within the FDA responsible for this outrageous lie. The WHO got in on the act by claiming IVM was ineffective, despite its own teams on the ground in Uttar Pradesh seeing proof of effectiveness amongst millions of people. What is the difference between a few humdred million in a study group and a few tens of thousands in a clinical trial? Probably around 2 billion dollars.
Even ignoring the reduction in R0 to zero from use of either HCQ or IVM treatment protocols, here is an illustration of the impact of HCQ and IVM protocols on the numbers of “cases” and “deaths with C19 present” on the course of the pandemic in the US, assuming an 80% effectiveness as a prophylaxis and early to mid-stage treatment:
Ivermectin for COVID-19: real-time analysis of all 184 studies (c19ivermectin.com)

It must be stressed that these numbers assume the 80% effectiveness on ALL new cases that all new cases with no impact on “floolow-on” imfectioms. Eradication of imfection leads to no further infections. In the case of Uttar Pradesh, cases went to zero. US cases of C19 would have been close to zero within one month of the distribution of IVM/HCQ protocols, as would deaths with C19 “present”.
There would also have been no need for injections. Neither would there have been the evolution of variants forced by, first, infections amongst those participating In the clinical and then, more importantly, by the roll-out of the injections.
Instead, the pandemic continued and ballooned out of control. The result was another 96.5 million “cases” and close to a million more “deaths with C19 present”.
Now for some data on the lethal toxicity of the injections.
Here is a table that shows the frequency of deaths, adverse events and life threatening events since the launch of the injections, shown before and after the adjustment for the under-reporting factor of 41.


The above table shows the number of doses for each death, event and threat to life.
Deaths per million doses are now approaching 1,000 per million doses, meaning that for every million doses, 1,000 people die. This rate has increased by 27% in the last 9 months.
Life threatening events are stable at around 870 per million doses, with a life threatening even occurring every 1,146 doses.
There are almost 60,000 adverse events per million from the injections, meaning that there is one adverse event per 18 doses.
The same calculations can be done for each adverse event, from Bells Palsy, Myocarditis, Blindness, Doctors Visits and so on.
Excess mortality data from Europe is around 20% in some countries. For the US, using this excess mortality number and applying it to pre-pandemic deaths in 2019, of 2,854,834, excess deaths are running at around 571,000 a year.
To sum up, instead of reducing cases and deaths to zero using IVM and HCQ protocols in May 2020, the corrupt, malicious or inept (or all three terms) WHO/FDA/CDC/NAIAD/NIH complex has killed more than 800,000 Americans and wounded close to 36 million – excluding preventable C19 injuries experienced by Americans over the course of the pandemic.
These numbers can be multiplied by 20 to apply globally, though EUDRA numbers are even more severe. A commenter (h/t Momo) on my post linked below, pointed out that German doctors are even less likely to report adverse events, estimating the URF at 70, rather than 41.
20 million saved or 20 million killed - by Peter Halligan (substack.com)
A few final points. In my post Vile Vials - by Peter Halligan - Peter’s Newsletter (substack.com) I pointed to the varying quality of the “vaccine” manufacturing process with deaths and adverse events up to 11x hSgher in some US states compared to others. This is a flagrant breach of the regulatory duties for quality control of the CDC/FDA. Just as outrageous as the treatment of the whistle-blower on the Ventavia clinical trial who was sacked for blowing the whistle. I doubt whether any of the other clinical trial sites dotted around the US and the rest of the world were of a higher standard. Why aren’t there more whistle-blowers at clinical trial sites? Are they too well rewarded for complicity?
Another post highlighted the monetary incentives for perpetuating CDC/FDA protocols. The massive environmental impact is ignored by all. It is not just the masks and needles that have an impact, but hundreds of billions if not trillions of wet wipes too. An Inconvenient Truth - by Peter Halligan (substack.com)
Of further interest, US federal authorities have been “outed” as promoting the “vaccine” narrative with tax payer dollars. Taxing US citizens whist promoting a FAKE C19 narrative requiring a toxic “vaccine”.
Judicial Watch Uncovers Biden Administration Propaganda Plan to Push COVID Vaccine | Judicial Watch
https://www.judicialwatch.org/covid-19-vaccine-campaign/
“Washington, DC) – Judicial Watch announced today that it received 249 pages of records from the Department of Health and Human Services (HHS) detailing the extensive media plans for a propaganda campaign to push the COVID-19 vaccine.”
References:
Coronavirus Graphs: Worldwide Cases and Deaths - Worldometer (worldometers.info)
VAERS Summary for COVID-19 Vaccines through 8/20/2021 – VAERS Analysis
VAERS Summary for COVID-19 Vaccines through 12/24/2021 – VAERS Analysis
Determining the VAERS Under-Reporting Multiplier (healthimpactnews.com)
Total COVID-19 vaccine doses administered per 100 people (ourworldindata.org)
Dr George Fareed and Dr Brian Tyson Early Treatment Protocol (2022) (onedaymd.com)
The last link is a cure.
From my layman’s perspective, the spike protein has some equivalence to a snake bite and might be cured with the equivalent of anti-venom. Snake anti-venom is developed in an animal host by repeated injections of venom to develop “super-immunity”. The relevant substances are extracted and injected into a snake-bit victim. Maybe this is a way forward for “long covid” and the “vaccine” injured. Any toxicologists out there? (Any association to a snake cult are purely coincidental!) I cannot understand the manufacture of cyto-toxins within the body, or reconcile the amount manufactured internally for months, compared to the injection dosage.
https://www.youtube.com/watch?v=fQDghpktskk
The FDA Misled the Public About Ivermectin and Should Be Accountable in Court, Argues AAPS