
Return of the ‘flu – or is that “Return of correct diagnosis of the ‘flu and pneumonia”?
Return of the ‘flu – or is that “Return of correct diagnosis of the ‘flu and pneumonia”?

Quick side note. A new “seeker of truth” has arrived on the scene in Canada, opencanada.info. It has an article out today that shows the risk to benefit ratio of children compared to the elderly.
Worth a read. Bottom line: 71 deaths with C19 present amongst children under 20 compared to 649 “serious” adverse events for a ratio of 9.14, compared to rates for over 20 year old adults of 49,541 deaths with C19 present and 9,870 “serious” adverse events for a ratio of 0.19.
“Serious” adverse events are life threatening – “Severe” are life altering.
The ratio of risk of a serious event from the C19 injections relative to deaths from C19 is almost 50 times greater (the article cites 100 times greater, so I may have missed something here).
Are adverse events reported from “vaccines” reported at higher rates than in the US, where somewhere around only one event is reported to VAERS for ever 40 suffered? Who knows. Here is a link to the Canadian adverse event reporting site.
Consider also that deaths with C19 present are NOT the same as deaths CAUSED by C19 and we know that the (early) Drosten RT-PCR test used to “diagnose” SARS-COV2 infections and hence C19 deaths were withdrawn because they could not distinguish between ‘flu and SARS-COV2.
Put it another way, had the Drosten RT-PCR test been used prior to the pandemic, almost all ‘flu cases would have been diagnosed as SARS-COV2 infections.
Lots more data and charts in the article and on the main site.
Right, having digressed a little, I went surfed some of the references in the article and went back down the rabbit hole of “where did the ‘flu go in 2020 and 2021” – which really begs the question “were all C19 cases really misdiagnose ‘flu cases, since the Drosten RT-PCR test was rubbish?”
From here: National Influenza Annual Report, Canada, 2020–2021, in the global context - Canada.ca
Here are charts for northern hemisphere ‘flu cases over the 2020 and 2021 ‘flu seasons for the US (LHS) and the EU (RHS)
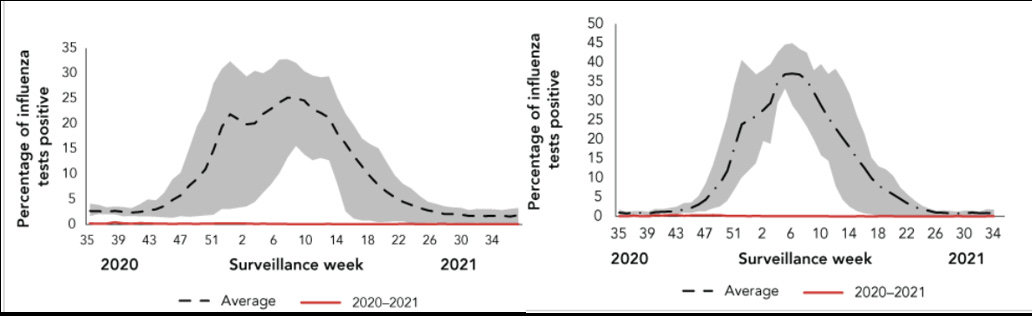
The orange flat line represents ‘flu cases over the 2020 and 2021 flu seasons. The grey areas above are averages of prior years and ranges for those years.
No ‘flu for two ‘flu seasons. Nada.
How about the southern hemisphere? Australia (LHS) and Chile (RHS.
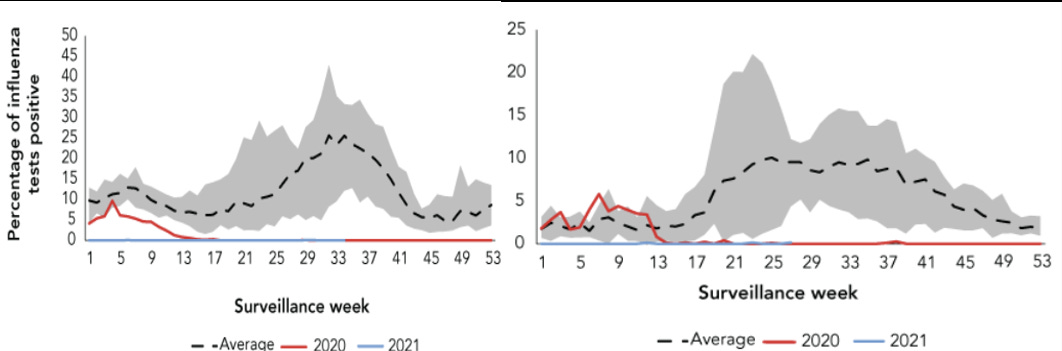
Same outcome. No ‘flu to be seen.
The source article shows more charts for testing for the ‘fu virus – no significant change from testing patterns from prior years over 2020 and 2021 ‘flu seasons.
No doubt there is some sort of analysis to be done that compares testing for ‘flu and testing for the SARS-COV2 virus that causes the C19 disease here.
All this leads to another question.
If there are zero ‘flu cases (yeah I know, there were but they were diagnoses as SARS-COV2 cases) what about pneumonia cases? Pneumonia is a lung infection that takes 2.5 million people a year, see here:
World Pneumonia Day - Stop Pneumonia / Every Breath Counts
“Pneumonia is the single biggest infectious killer of adults and children – claiming the lives of 2.5 million, including 672,000 children, in 2019.”
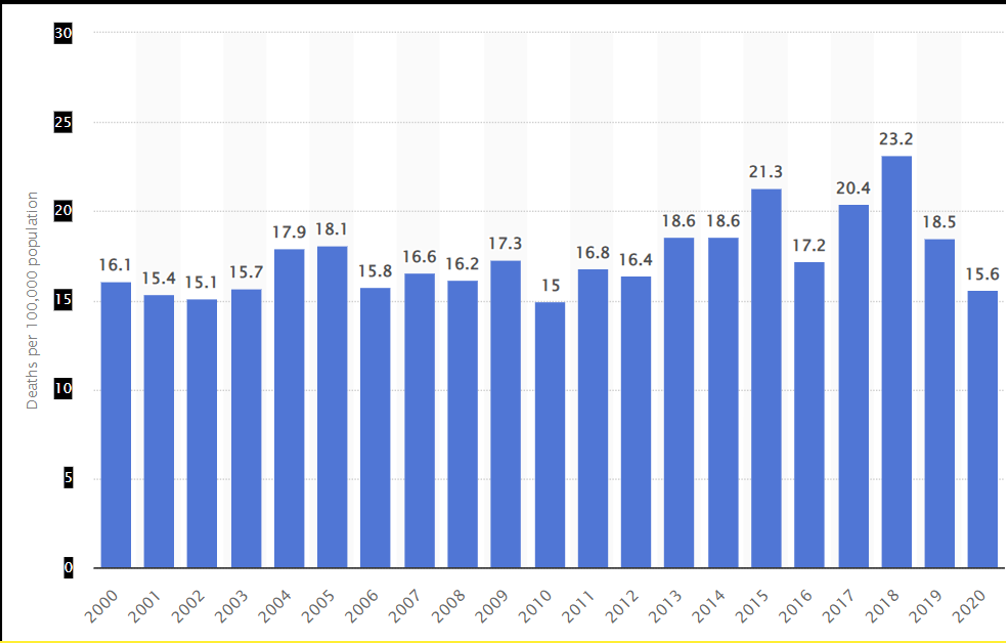
There was no significant change in 2020 pneumonia deaths in Canada relative to deaths earlier this century, but they are down from a “spike” in 2018 here:
Note: since there were no flu deaths in Canada over 2020 and 2021, ALL the deaths in 2020 here are pneumonia deaths.
Death rate for influenza and pneumonia in Canada from 2000 to 2020(per 100,000 population)
The WHO does not consider pneumonia a “Public Health Emergency of International Concern” (PHEIC pronounced FAKE) despite the fact it has taken more lives than the (misdiagnosed using Drosten RT-PCR tested) three year C19 pandemic (6.7 million with C19 “present” v 7.5 million from pneumonia). Pneumonia is treatable with antibiotics. Rather, the WHO conflates misdiagnosed C19 “cases” with correctly diagnosed and treatable (with antibiotics) pneumonia.
The WHO recommends AGAINST the use of antibiotics for C19 because it interferes with possible C19 treatments and recoveries. See the interview below with a WHO official Dr Hanan Balkhy.
Episode #11 - Antibiotics & COVID-19 (who.int)
“It's very important to realize that we do not need to give antibiotics to patients who are isolated with COVID-19 in their homes, because they have mild disease. And, to only be receiving antibiotics if they are significantly ill, where the healthcare provider is suspicious of – on top of the COVID-19 – the patient having a bacterial infection. And, this needs to be done by a prescription of a healthcare provider.”
Problem is, if a patient has pneumonia and is misdiagnosed as having C19, because of rubbish Drosten RT-PCR testing, withholding antibiotics that would cure the infections may be a death sentence.
How many people died from (untreated with antibiotics) pneumonia that were categorized as C19 deaths? If the Drosten RT-PCR test could not distinguish between different ‘flu viruses and strains, could it differentiate between lung infections from pneumonia and C19 disease?
Now there is a valid concern that over-use of antibiotics leads to the equivalent of “immune escape” of the bacteria causing infections – see ND4 infections – but, right now, antibiotics work. If they stop working, or their decreasing utility can be “triaged”, their use is essential.
Onwards!
I drink a lot of coffee – if you like my “stuff” but don’t want to pay for a subscription you can buy me a cup to show (any!) appreciation here: https://ko-fi.com/peterhalligan
My vote is the later. "Covid" was a well marketed flu. (Dr. Vernon Coleman). People didn't fall over dead in the streets (as it was implied they would). But they are now, the bio-weapon shots are doing that. The average age of death "from covid" is close to life expectancy. I wonder what happens when you are about to die and you get a flu?
I wonder what happens when you get the flu and have 1-4 co-morbidities, given Remdesivir and respiratory suppressing drugs. Hmmm.
The C19 vax cures pneumonia!