Some suggested metrics for clinical trials – some rambling thoughts

First let me say any clinical trials must not be unblinded and must be fraud free – unlike the Phase 3 Pfizer C19 mRNA clinical show trials.
The Canadian Covid Care Alliance (CCCA) performed an analysis of the Phase 3 Pfizer show trial here over a year ago. Others have conducted similar analyses.
The COVID-19 Inoculations - More Harm Than Good FINAL Video & Print (canadiancovidcarealliance.org)
On pages 11 and 12 we have these tables:

Please check out all 51 slides. Or view a video here:
The Pfizer Inoculations For COVID-19 – More Harm Than Good – VIDEO – Canadian Covid Care Alliance
There is no easily found follow-up data on the show trial participants after, say, 6 months or a year to see whether they were reinfected or became sick or died.
Secondly, alternative treatment protocols need to be run in parallel to experimental mRNA injections to compare outcomes over the short, medium and long terms.
Big pharma should be made to pay for at least half a dozen of these studies that would probably cost around 50=100 million each. They would not even notice such a cost out of the tens if not hundreds of billions of profit they have made in “blood money”. Call it a “carbon tax” as this would be as appropriate as the huge taxes levied on hydrocarbon companies for no good reason.
The sole objective of the clinical show trials was to prevent severe symptoms – remember all the fear about “cytokine storms”? Cytokine storms were the source of the “fear is the mind killer” propaganda that was hyped to the maximum at the outset of the pandemic and disappeared as a tool to scare people witless over just a few months into the summer of 2020.
Perhaps there were no such cytokine storms in either the control or placebo groups over the period of the show trials that were scheduled from 31 July 2020 to 31 January 2021.
The point is, the sole end point for the show trial for the Pfizer mRNA and other injections was to demonstrate efficacy in preventing severe symptoms of C19 – NOT preventing infection or transmission, NOT preventing hospitalization and NOT preventing death.
Moving on to some suggested metrics to evaluate the safety and efficacy of the clinical show trials.
These metrics must compare the differences between an estimated benchmark, or base-line, and the estimated path without interventions and the estimated path – using clinical trial data – with interventions.
Keep in mind that the this is the actual path of the pandemic – using intentionally inaccurate and fraudulent measures of “cases” and “deaths with C19 present”. This is the WHO defined coirse of the pandemic that is currently being written into the laws of every country in the world. None of those amending the regulations in the IHR 2005 or the new Pandemic Treaty have any expertise in preventing or solving pandemics – no successful track records whatsoever.
Data sourced from here:
Coronavirus Graphs: Worldwide Cases and Deaths - Worldometer (worldometers.info)
84 million “cases” before the roll-out of C19 injections, 687 million “cases “after the injection roll-out – with “cases diagnosed” with the unfit for purpose Drosten RT-PCR test. An increase of more than 600 million “cases” – more than 8 times the number of cases after C19 injections compared to the number before C19 injections.
1.3 million deaths with C19 present before C19 injections – 6.9 million deaths after the roll-out of C19 injections – an increase of 5.6 million – an increase of more than 5 times with C19 injections, compared to with no injections.
What sane person anywhere in the world would deny the complete and utter abject failure of the pandemic response? 8 times the cases and 5 times the deaths AFTER C19 injections compared to BEFORE C19 injections. And that is before C19 injection harms are taken into account.
Now factor in that the majority of deaths with C19 present were not caused by C19 but were in fact caused by “death by healer” – the withholding of existing treatments, the non-diagnosis of emerging deadly non-C19 conditions, the use of Remdesivir, Midazolam+morphine, the deprivation of food and water from hospitalized patients, the failure to allow anti-viral treatment protocols such as IVM or proven HCQ treatment protocols and last, but not least, the instructions from the WHO to withhold anti-biotics as they would interfere with the course of the disease and treatment with injections.
Remember there have been no studies on the impact of C19 mRNA injections on the safety and efficacy of treatments used for non-C19 related conditions. Not for cancer treatments, treatments for diabetes, depression, Alzheimer’s, heart conditions – nothing on the INTERACTION of C19 mRNA or viral vector injections at all.
I am still at a loss as to how prioritizing the elderly and infirm who have non-existent or severely impaired immune systems, for injection with instructions to create a toxin (and with toxic delivery mechanism) can possibly be expected to generate an immune response from the non-existent or severely impaired immune system. The assumption is that, somehow, the C19 injections resurrect the dead and impaired immune systems. There is bags of research that shows the immune system is impaired by the C19 injections and yet BOOSTERS are still recommended by health regulators for the elderly and “at risk” population. Perhaps someone can enlighten me as to how this can possibly make any sense.
The medically and scientifically unqualified “shiny-trouser bottomed” diplomats and bureaucrats drafting amendments and treaties have nothing to say about the failures of every single measure imposed by the WHO and implemented by governments – equally unqualified – who threw out decades of learning and evidence based medicine about pandemic measures – to impose their bureaucratic, political (not medical or scientific) will on those deserving of their protection.
Ok. Let me reintroduce a couple of key metrics.
Life Years Lost (LFY) and Number Needed to Vaccinate (NNV).
LFY can be estimated for the course of a pandemic with and without intervention. There are many who say that this should be improved by viewing Quality LFY (QLFY) in some sort of triage approach. The cynical amongst us might argue that a definition of QLFY was adjusted to reflect possible cost savings and the allocation of hospital/medical resources – that is, “quality” was correlated to metrics used to determine eligibility with assisted suicide criteria in countries like Canada, the Netherlands and Switzerland. Prior metrics, such as the ability to walk 20 meters unassisted and pain free, were extended to 100 meters – and so on and so forth. A topic for another day.
It is easily possible for any hospital, employer or church to compile this sort of data by surveying groups of people they encompass. This could be done before and during the pandemic with and without C19 injections.
A version of LYL and QLYL was bastardized by the chief mongrel at the Imperial College of London, “Professor” Neil Ferguson. It is my view that Ferguson formulated the outcomes that would cause panic and only then wrote the computer model that would provide those scary outcomes. I am of the view that same logic was applied in designing the Drosten RT-PCR tests – set the outcome, then design the test to meet it.
Sample populations based on age, sex, income, colour or whatever can be created in clinical trials or sample populations to measure the path before and after any measures – such as lockdowns, masking, social distancing, vaxx passports, injections or other treatment protocols.
Where deviations from clinical trial outcomes exceed rational parameters, the treatments should be stopped until such a time as the reasons are either recognised as excessively adverse or tolerable – with full disclosure to enable informed consent.
Number needed to Vaccinate
Combing some key data from the UK and US, it has been revealed 125,000 people need to be injected in order to prevent a single Intensive Care Unit admission in the UK with C19 – amongst the population not at risk (not elderly or with significant co-morbidities).
At the same time, in the US, an emergency admission as a result of C19 mRNA injections was calculated at one admission per 800 people injected (one in 600 for Moderna and one in more than 900 for Pfizer/BioNTech).This sort of data can be verified and compared by looking at V-Safe data for 10 million people released a few months ago and used to estimate the under-reporting factor for VAERS for non-death injuries here:
The implication of combining these two numbers couldn’t be clearer. Inject 125.000 people with C19 injections and cause 156 emergency hospital visits in order to prevent one ICU admission from C19.
This NNV metric can be applied to any demographic in order to provide informed consent.
So there are two important and easily derived metrics that facilitate informed consent to any demographic. They fly in the face of the “one size fits all” approach mandated in many countries on the instructions of the WHO, which in turn discarded decades of medical and scientific evidence about to be enshrined in amendments to IHR 2005 and a new Pandemic Treaty – all enforced with a Nazi party style “papers please” international health passport. Note, you will not be able to travel anywhere without a “health passport” so it is a de facto global ID system.
Time and Frequency of all candidate treatments with a sufficient track record
By now, we are all aware that the majority of “spontaneous” reactions – including death – to the C19 injections occur within 14 days of the injection. Bottom chart here:
COVID Vaccine Data - OpenVAERS
There are a host of other treatment protocols – like IVM and HCQ, Vitamin supplements and e.g. Melatonin, Nigella Sativa and Aspirin – that do not result in death within 14 days of use.
You can view these alternatives and the studies that support them here (cruise around the site to view them, don’t just stick with the Ivermectin studies on the splash page):
Ivermectin for COVID-19: real-time analysis of all 204 studies (c19ivm.org)
Corrupt regulators and big pharma state that you are not inoculated until 14 days have passed – ergo the claim is that all deaths and adverse events within 14 days cannot be due to the injection. (Note the flip-side – the WHO states that anyone who died within 28 days of a positive C19 death must have C19 attributed as cause of death on death certificates and in statistics – even if it’s food poisoning, gunshot, vehicle accident or cancer. This is falsification of data by the WHO and by all countries health regulators).
There are plenty of statistics from a whole host of countries that show that C19 was responsible for around 5% of deaths currently classified as deaths from C19. C19 may or may not have been present at time of death, using the unfit for purpose Drosten RT-PCR test, but 95% of people reported to have died with C19 present, did not die from C19.
In other words, instead of the 6.8 million reported globally to have died with C19 present, less than 350,000 died with ONLY C19 present. For the US, instead of 1,160,000 deaths with C19 present, fewer than 60,000 died with ONLY C19 present. Ninety fiver per cent of those that died with C19 present had 2-6 other conditions already killing them and were also 1-2 years older than average life expectancy.
In the future, we need informed consent. The clinical show trials tested two dose regimens that were supposed to last years, if not decades. Now we are faced with the prospect of these failed injections being required every few months, with variants being forced, that by-pass any targets with increasing ease.
It should be clear before the injections are administered, how long the injections are proven to be effective. If it is for a 3 months or a year or unknown because of the likely emergence of new variants, this should be stated at the outset.
There have been no clinical trials performed anywhere in the world for the impact of more than two monovalent doses of the C19 mRNA injections, or bivalent booster doses administered once, twice or more times on top of the two monovalent doses of the “initial series” or multiple doses of the bivalent doses.
In other words, with no clinical evidence to support continued administration, there is no evidence that one booster every three months or every year, or every two years or any period has the correct dosage or any likelihood of durability.
It is a medical fact that dosage is a determinant in treatment that can kill or cure – same as for “recreational” drugs- overdoses are lethal.
Evidence based medicine requires that the duration of efficacy and frequency of treatment need to be known in advance and based on honest clinical trials.
Interaction of a range of possible treatments, not just a mRNA injection
From the show trial demographics shown on pages 15-17 of the CCCA report, it is apparent that there was no consideration for the INTERACTION with drugs being administered to the elderly and infirm for say diabetes, Alzheimer’s, ADD, depression ,autism, leukaemia, cancer, heart disease and so on. The implicit assumption is that the C19 injections would provoke an immune response in the already mostly destroyed immune systems of the elderly and infirm – the C19 injections would somehow “resurrect” a failed immune system. How it could possibly make sense to inject a toxin into the elderly and infirm is beyond me. The clinical show trial was mostly tested on the health BUT PRIORTIZED for the elderly and infirm at the outset of the C19 injection roll-out.
Separate and distinct clinical trials for each potential reaction to an existing treatment must be conducted in order to establish and adverse reactogenicity of interactions with existing treatments.
One of my first SubStack posts suggested that there were techniques in the field of investment management that could be applied to the field of treatment protocols in medicine.
Here’s how.
1. Clean the data of the fraud perpetrated by health regulators (14 days before inoculation, diagnosis of “cases” with accurate (not RT-PCR or RAT tests) testing, using death statistics with ONLY C19 present. Extending the clean up of data to leading causes of death.
2. Compiling baseline data for every important demographic (age, sex, color, income etc) using, say, 2015 to 2019 as a benchmark for each category.
3. Compare 1 with 2 to examine changes per category and compare with clinical trials.
This is a “first order” analysis. Let’s move on to more detailed work – again, not the best, but a move in the right direction.
Investment managers will be familiar with a technique called “Benchmark Relative Performance Measurement and Attribution”.
For (usually monthly) periods, the return from an investment portfolio is compared to a benchmark. The benchmark is set and the investment manager can used bounded discretion to vary benchmark weights to different sectors and also take positions within sectors.
The formula to determine value added or lost is below:
Asset Allocation = relative weight times sector index return (e.g. a “contribution” to return can be calculated if an overweight position was taken in a sector that out-performed the overall benchmark return – so if there was a 10% overweight to US equities that beat the overall benchmark return by 5%, the “contribution” to performance was +0.5% and has a dollar equivalent of +0.5% times the starting total market value of the overall portfolio.
Sector Selection – this is equal to the benchmark weight of the sector times the difference in return between the actual return for the sector less the index return for the sector. For example, if the benchmark weight for Japanese bonds is 10% and the Japanese bonds in the portfolio out-performed the Japanese bond index by 0.5%, the contribution to the overall portfolio excess return is 10% times 5% - which has a dollar equivalent.
Interaction – the relative weight times the relative return for each sector, expressed in percentage and dollar terms.
Summing the dollar amounts across each sector by these three dimensions of Asset Allocation, Stock Selection and Interaction provides the value added or lost by the investment manager for each decision to deviate from the benchmark by month, quarter and year.
This same benchmark relative performance measurement and attribution can be used for any treatment protocol and demographic.
Another investment and banking technique used to quantify risk is called “Value at Risk”. Value at Risk is usually expressed as “in the next month, there is a 5% chance you will lose this much money” based on the historical risk characteristics of the current holdings”.
It can represented as below, taken from here:
Value at Risk - Learn About Assessing and Calculating VaR (corporatefinanceinstitute.com)
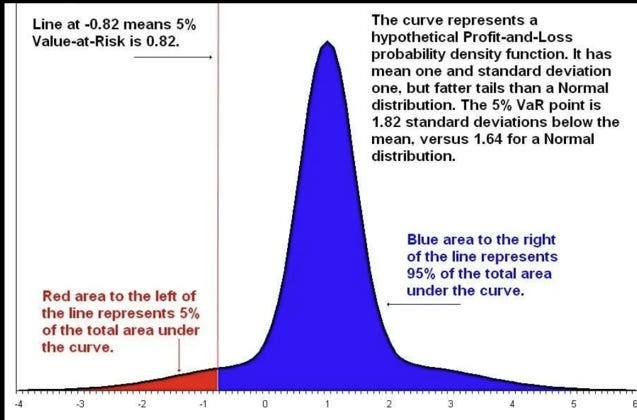
Everything in blue is, more or less, an acceptable outcome. (Not death!).
The left hand tail of the probability distribution curve represents the estimate of maximum loss.
The Value at Risk can be re-stated as “Lives at Risk” and a deep dive into that tail completed to see how this can be mitigated.
A key issue here if the use of ex-post and ex-ante risks plus the statistical signifcznce of data. Ex-post is a measure of PAST variability of actual returns – so is a matter of fact.
Ex-ante is an estimate of current risk, using the current (not past) holdings. It is NOT a forecast.
A measure of the quality of the investment manager is how close the ex-post risk (variability of returns) correlates with the ex-ante volatility of returns – since it indicates that risk is not only measured accurately, but also is managed accurately.
Even more advanced risk management techniques can be derived to engage in “benchmark relative VaR”, but let’s leave that for now!
Ok, a lengthy post, but I hope it signals how a move to quality of data and its interpretation is not only possible but is being used elsewhere to achieve measurable and important analysis of outcomes. You would think that in these days of gigabit per second processing of data using algorithms and artificial intelligence that someone would come up with positive applications rather than the expensive damage and/or replacement of human body parts!
Onwards!
Please upgrade to paid, or donate a coffee (I drink a lot of coffee) - “God Bless You!” if you can’t or don’t want to contribute. Coffee donations here: https://ko-fi.com/peterhalligan - Buying just one Ko-fi a week for $3 is 50 bucks more than an annual $100 subscription!
We’ll done Peter. It seems to me, given what has been observed and revealed over the last 3 years, that the most economical way to true up the data would involve a return to honesty. However, our current brokers have eliminated that backstop. We peer through bits and pieces of data not unlike the weekly crossword. Let’s see if we can figure it out. The cost of “what we allow” is unsustainable. Pressure and time. It’s time to make the diamonds. 😉
IMAGINE A CAR THAT BLEW UP ONE IN TEN THOUSAND TIMES
IMAGINE A RESTAURANT THAT POISONED YOU ONE IN TEN THOUSAND TIMES
VACCINES ARE A MEDIEVAL DELUSION FROM AN ERA OF BLOODLETTING, FULLY 60 YEARS BEFORE DOCTORS AGREED TO WASH THEIR FRIKKIN HANDS YOU FOOLS.
INJECTING 'DIS-EASE" PAST YOUR NATURAL DEFENSES TO PROTECT YOU IN CASE IT SOMEHOW GETS PAST THEM IS NONSENSE AND INSANITY ON ITS FACE
WAKE. UP.
PARANOID SCHIZOPHENIC PSYCHOPATHS ATTACK YOU OVER THINGS ONLY THEY CAN 'SEE'
READ JANINE ROBERTS' EXCELLENT BOOK 'FEAR OF THE INVISIBLE'
AAAAAAGGGGHHHHHH
https://Fearoftheinvisible.wordpress.com