
Some thoughts on RT-PCR, lateral flow testing and the S1 and S2 spike protein components
Some thoughts on RT-PCR, lateral flow testing and the S1 and S2 spike protein components

RT-PCR testing has been used to detect the presence of SARS-COV2.
From here:
Gene-Target Strategies for SARS-CoV-2 RT-PCR Testing | ZYMO RESEARCH – Zymo Research International
“DETECTION DETAILS
SARS-CoV-2 targets commonly detected by rRT-PCR tests include the nucleocapsid (N), envelope (E), spike protein (S), RNA‐dependent RNA‐polymerase (RdRp, also known as nsp12), and open reading frame1ab (ORF1ab) genes 1. N, E, and S are structural proteins while RdRp and ORF1ab are important for the replication of viral RNA. The N protein packages viral RNA into a helical nucleocapsid, the E protein forms a structure that encloses viral RNA, and the S protein consists of glycoprotein spikes that facilitate the invasion of host cells (2).”
My ignorance I am sure but this confirms to me that the mRNA injection process entirely replicate the injection process. Meaning that injection and infection are entirely fungible. But, what do I know!
I note there is no differentiation of S1 and S2 – just a referral to “S”.
Note (2): “2. Significance and Difference between Target Regions for SARS-CoV-2. PerkinElmer Applied Genomics. Published 2020 Apr 12. https://perkinelmer-appliedgenomics.com/2020/04/06/significance-and-difference-between-target-regions-for-sars-cov-2/”
Kevin McKernan stated that the S1 exists only on the infection, whereas the mRNA injection shows S1 and S2 and both can be delineated – meaning that “long C19” can be distinguished from “long vaxx” injuries and deaths.
We have this from Australia here – poor buggers got a lot of Oxford/Astra Zeneca:
“Do the vaccines give you COVID, or make you test positive for COVID? Does the vaccine affect other tests? Do we still need to get COVID tested if we have symptoms, even after getting the shot? And will we still need COVID testing once more of the population gets vaccinated?”
“2. Will the COVID vaccine make me test positive?
No, a COVID vaccine will not affect the results of a diagnostic COVID test.
The current gold-standard diagnostic test is known as nucleic acid PCR testing. This looks for the mRNA (genetic material) of SARS-CoV-2, the virus that causes COVID-19. This is a marker of current infection.
This is the test the vast majority of people have when they line up at a drive-through testing clinic, or attend a COVID clinic at their local hospital.”
Check out the answer to question 1 as well “1. Will the vaccine give me COVID? The short answer is “no”. That’s because the vaccines approved for use so far in Australia and elsewhere don’t contain live COVID virus.” I think this needs to be fact checked by someone outside the mis-“Trusted News Initiative” – the truth, the whole truth and nothing but the truth would re-pose the question “is the injection more or less likely to make me contract COVID”.
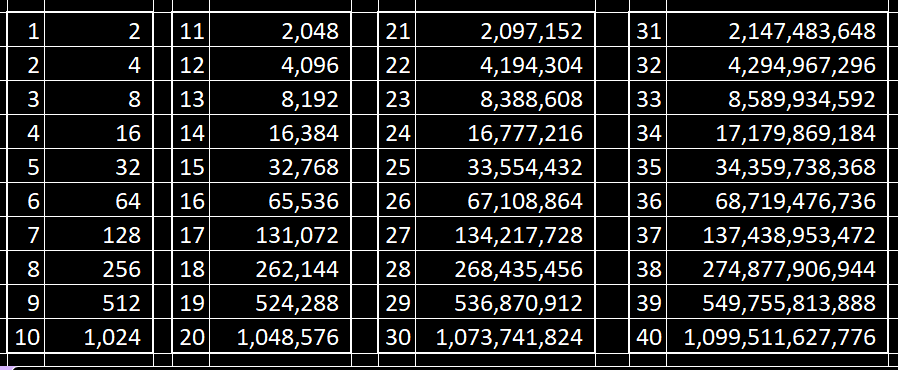
Okay, lets show a table of number of magnifications per cycle used in RT-PCR tests:
From here:
PCR Amplification | An Introduction to PCR Methods | Promega
“Basic PCR - .. Each PCR cycle theoretically doubles the amount of targeted sequence (amplicon) in the reaction. Ten cycles theoretically multiply the amplicon by a factor of about one thousand; 20 cycles, by a factor of more than a million in a matter of hours.”
Here is a cycles v amplification table.
I confess, I had not associated Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) with the actual process of manufacturing DNA into modified mRNA until I watched the three hour special yesterday!
Urgent Expert Hearing on Reports of DNA Contamination in mRNA Vaccines (worldcouncilforhealth.org)
I suspect that three hour video will prove to be a turning point in history – let’s hope the meeting of minds blossoms until it permeates every aspect of the regulatory approval process around the world. Certainly the WHO and country regulators need to watch it – twice, if not three times!
For contaminants in the C19 mRNA vials, Kevin McKernan stated that just 17-24 cycles were needed – that is, magnification of 131,072 to `16,777,216 times was required to detect the contaminants.
For those RT-PCR tested, cycles of between 30 and 40 were used – that is, magnification of between a billion and a trillion was used (40 is generally the maximum “threshold” of detection of fluorescence if my understanding is correct).
Okay, one last observation from here:
Did Operation Moonshot inadvertently reveal the pseudo-pandemic? (substack.com)
“The £200bn UK moonshot programme selected the Innova LFT. Unlike PCR this test did not inflate SARS-CoV-2 positives and thus revealed that 2020 through to 2021 was a pseudo-pandemic.”
LFT = Lateral Flow Test
“At the time few noticed how important this gap between LFT and PCR positivity was, or commentators still wrongly believed that PCR could be trusted in the right hands and simply ignored the low SARS-CoV-2 positivity from LFT tests.
The deployment of the Innova LFT may have inconveniently highlighted how bad the PCR testing was and how inflated the PCR positive numbers were, thus revealing very low SARS-CoV-2 positivity rates.
‘Coincidentally’ the FDA demanded the Innova LFT be withdrawn from the US market in 2021, despite it being the largest investment in a single medical test from a single manufacturer in human history.”
A better test was turned down by the FDA/CDC because it (correctly?) returned to many negatives, this contradicting the narrative of “fear and loathing, and panic” that was desired by the FDA/CDC????
Which leaves me with a few articles from a few years ago that make me go “Hmmm” and struggle with the impulse to seek more coffee.
SARS-CoV-2 Spike Protein Extrapolation for COVID Diagnosis and Vaccine Development - PMC (nih.gov)
“The spike glycoprotein (S-protein), anchored onto the virus envelope, is the trimer of S-protein comprised of S1 and S2 domains which interacts with host cell receptors and facilitates virus-cell membrane fusion. The S1 domain comprises of a receptor binding domain (RBD) possessing an N-terminal domain and two subdomains (SD1 and SD2). Certain regions of S-protein of SARS-CoV-2 such as S2 domain and fragment of the RBD remain conserved despite the high selection pressure.”
Ok, so S2 existed on the S-protein of the virus – which means that the fact that the S2 in the mRNA injections cannot be the same as the virus – if it can be identified by manufacturer and number of doses.
And stuff from the EU and WHO here:
Available methodologies methods for monitoring SARS-CoV-2 variants of concern (europa.eu)
“The only way to identify and characterise new variants and unambiguously type existing variants is with genomics. Guidance on sequencing of SARS-CoV-2 can be found in ECDC’s technical guidance Sequencing of SARS-CoV-2 and the WHO’s Genomic sequencing of SARS-CoV-2: a guide to implementation for maximum impact on public health “
Lastly, all the work done so far to determine levels of toxic contamination in the C19 mRNA injections relates to Process 1 (clinical trials – which had “more harm than good” with the cure worse than the disease by a wide margin AND Process 2 – a poorly made and completely different product. Process 3 – a change made by the manufacturers that needed no regulatory approval of justification – remains to be done.
Time for coffee!!!
Onwards!
Please buy a subscription or donate a coffee (I drink a lot of coffee) - “God Bless You!” if you can’t or don’t want to contribute. Coffee donations here: https://ko-fi.com/peterhalligan - an annual subscription of 100 bucks is one third less than a $3 coffee a week!
I believe these studies of equine influenza, PCR testing and vaccines contain many answers we are seeking.
In reading them you will see that flu vaccines will cause flu outbreaks. You will see that the PCR tests are capable of detecting exactly which strains are derived from specific vaccines, identifiable from wild type flu.
The information from veterinarian studies is less censored because it's less politically charged. But it's exactly the same applied biotechnology and procedures. Cross-applied for both horses and humans.
Multifocal outbreak of equine influenza in vaccinated horses in Argentina in 2018: Epidemiological aspects and molecular characterisation of the involved virus strains
Equine Veterinary Journal, May, 2020
https://pubmed.ncbi.nlm.nih.gov/31494962/
Potential of vaccination to confound interpretation of real-time PCR results for equine influenza
The Veterinary Record, September 3, 2014
https://pubmed.ncbi.nlm.nih.gov/21813581/
Diagnostic methods applied to analysis of an outbreak of equine influenza in a riding school in which vaccine failure occurred
Veterinary Microbiology, June 10, 2003
https://pubmed.ncbi.nlm.nih.gov/12713892/
Detection of modified-live equine intranasal vaccine pathogens in adult horses using quantitative PCR
The Veterinary Record, November 22, 2014
https://pubmed.ncbi.nlm.nih.gov/25274853/
Diagnosis of equine influenza by the polymerase chain reaction
Journal of Veterinary Diagnostic Investigation, January 6, 1994
https://pubmed.ncbi.nlm.nih.gov/8011780/