

Worried world: “How much myocarditis risk was there in the bivalent shots?” – CDC: "It’s a secret, we will let you know if we think it’s important” – “What becomes of the broken hearted?"

A continued refusal by the CDC to provide the information required for informed consent has extended to the bivalent shots authorised on 21 August 2022.
The attitude of the CDC is reflected in this comment about releasing up to date information from its Vaccine Safety Datalink, which it prefers as an indicator of harms, rather than VAERS:
"What I was conveying is that in the era of the bivalent vaccine, the number of cases has fallen to where it no longer is giving a signal that is detectable," Dr. Pavia, chief of the University of Utah's Division of Pediatric Infectious Diseases, told The Epoch Times in an email. In response to how he could say that with the missing VAERS data, he said "the strongest data are from the controlled studies like the VSD where you have built in controls."
Built in controls huh? That’s nice. Presumably these controls take the form of filters that eliminate too much bad news!
Okay, what is the VSD? From here:
Vaccine Safety Datalink (VSD) | VSD | Monitoring | Ensuring Safety | Vaccine Safety | CDC
“The Vaccine Safety Datalink (VSD) is a collaborative project between CDC’s Immunization Safety Office, integrated healthcare organizations, and networks across the United States.
The VSD started in 1990 and continues today to monitor the safety of vaccines and conduct studies about rare and serious adverse events following immunization.
As of September 28, 2022, there are 13 VSD sites that provide clinical, methodological, and data expertise; 11 currently are data-providing sites and the remaining sites provide subject matter expertise.”
13 VSD sites as of a year ago. Is there any VSD on myocarditis from C19 injections? Well yes, though it is a little dated and relates to the old monovalent C19 mRNA injections.
Here is a study on myocarditis from the above site that covers the first 12 months of the old monovalent injections:
“Members 18-39 years of age at eight integrated healthcare-delivery systems were monitored using data updated weekly and supplemented with medical record review of myocarditis and pericarditis cases.
Incidence of myocarditis and pericarditis events that occurred among vaccine recipients 0 to 7 days after either dose 1 or 2 of a messenger RNA (mRNA) vaccine was compared with that of vaccinated concurrent comparators who, on the same calendar day, had received their most recent dose 22 to 42 days earlier. Rate ratios (RRs) were estimated.. “
Somewhat limited? Here’s an extract from some of the results:
“From December 14, 2020 - January 15, 2022 there were 41 cases after 2,891,498 doses of BNT162b2 and 38 cases after 1,803,267 doses of mRNA-1273. Cases had similar demographic and clinical characteristics. “
Right – a full 13 month period starting on the authorization date.
“During days 0-7 after dose 2 of BNT162b2, the incidence was 14.3 (CI: 6.5-34.9) times higher than the comparison interval, amounting to 22.4 excess cases per million doses; after mRNA-1273 the incidence was 18.8 (CI: 6.7-64.9) times higher than the comparison interval, amounting to 31.2 excess cases per million doses.”
Which led to this conclusion:
“Conclusions: Both vaccines were associated with increased risk of myocarditis and pericarditis in 18-39-year-olds. Risk estimates were modestly higher after mRNA-1273 than after BNT162b2.”
Maybe this was a study with far worse outcomes than another secret study on the incidences of myocarditis from the bivalent injections? Did the new bivalent study use VSD data from all 13 sites or new ones for just 18-39 year olds or for all age groups?
The point remains, there is going to be a bunch more VSD data for all age groups from probably more than 8 sites and for a full one year period for the bivalent shots and the CDC considers that the information is not suitable or relevant for people to look at to get the information they need to consent to the old bivalent injections or use it to base a decision for the new monovalent injections.
“Asked for more current data, the spokesman acknowledged the agency has it but is not making it public.”
"When appropriate, the updated safety data will be published," the spokesman told The Epoch Times in an email.”
Anyway, back to the bivalent/myocarditis story.
56.2 million doses of the bivalent shot have been administered – and have been replaced by what is intended to be an annual or bi-annual monovalent shot targeting XBB variants – unless bivalents are needed to target emerging variants every six months or a year from now on in.
From here:
“The CDC has acknowledged that heart inflammation is a complication of mRNA COVID-19 shots and, yet, the only published data released by CDC officials about that complication is a seven week study that ended on Oct. 23, 2022.
Where is more specific myocarditis/pericarditis data related to bivalent COVID shots for the past 10 months?" Barbara Loe Fisher, co-founder and president of the National Vaccine Information Canter, told The Epoch Times via email.”
Seven weeks prior to Oct 23, 2022 would be from the authorization date of 31 August 2022
So, a seven week study for the bivalent shot that is now obsolete and has been replaced by another experimental and unproven monovalent shot.
Barbara Lee Fisher wants to know the safety of the bivalent shot (not even relative to the original monovalent shot!) for the full period of use – more than a year – not just the first 7 weeks.
VAERS has some data:
“Through Sept. 8, 98 cases of myocarditis, pericarditis, or myopericarditis were reported to VAERS following bivalent vaccination, according to a search of the system by The Epoch Times.”
That would be 98 cases in a year and a week – to which one could apply an under=reporting factor of maybe 30 or 30.
So, what’s the beef?
Well it turns out that the CDC has another system that monitors adverse events. It is called Vaccine Safety Datalink.
“Dr. Nicola Klein, a Kaiser Permanente doctor who works closely with the CDC, gave a presentation (pdf) on COVID-19 vaccine safety. She presented data from the Vaccine Safety Datalink, a monitoring system that covers a much smaller population than VAERS.”
Here is the referenced (80 page) pdf:
It has this chart on page 14 of 66 in pdf format:
VSD COVID-19 RCA Surveillance: Outcomes Monitored Due to Emerging Concerns

No mention of reports on bivalent injections in that bottom few rows.
There is this chart on page 18 of 66

And these conclusions in the Myocarditis/Pericarditis section.

Data through June 2021. Humph"!
I haven’t read the whole report. There are 89 mentions of bivalent. 76 mentions of myocarditis and 75 mentions of pericarditis!
There is this table on page 50 of 66:
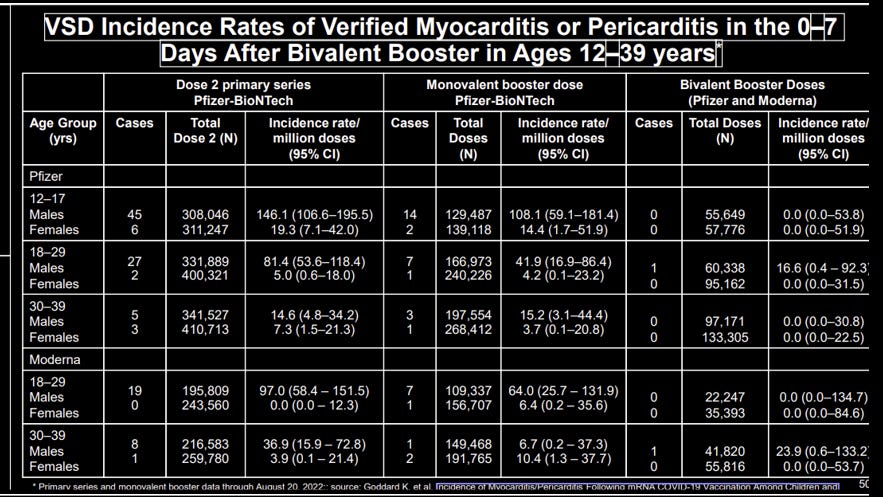
Read the rows for the Pfizer and Moderna numbers – presumably the column headings are subordinate to the row headings or this table is a “max and match” of injections?
The old monovalent male/female incidence rates per million is remarkable for the monovalent injections except for the 30-39 year Moderna booster doses. Which makes me thing this data needs closer scrutiny!
The disproportionate impacts towards males disappears to a slightly higher number of females to males for the booster shots of the same bivalents. Interesting!
Page 60 of 66 has this:
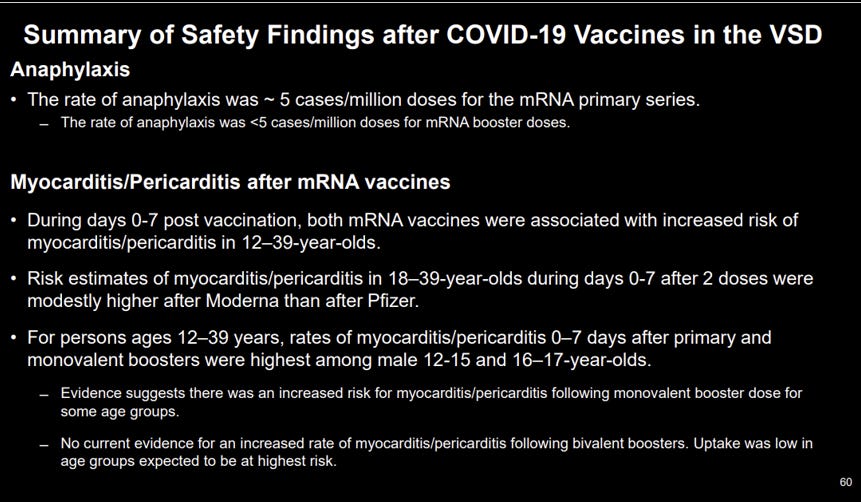
Just the one (bottom) liner about bivalents “low uptake amongst highest risk age groups”.
Other data is there on ischemic stroke on page 61:

A 59% higher risk of ischemic stroke of the Pfizer bivalent relative to some flu vaccine or other? No clue as to the relevant health condition of the two comparator groups to come to that conclusion that I spotted!
Ok, so that’s some “stuff” from the KP presentation to the CDC. How was this discussed by KP’s Dr Klein?
“Dr. Klein said that two cases of myocarditis after bivalent vaccination were detected in the Vaccine Safety Datalink (VSD) through March 11. It's not clear why more current data were not presented. Dr. Klein did not respond to a request for comment. The cases did not trigger a safety signal among adults, Dr. Klein said.”
Two cases on VSD to March 11t, presumably March 2023 and for the 6 and a half months since 31 August 2022 – where is the data for the 6 months since?
How did the CDC panel react?
“Panel members were taken by the data. Dr. Oliver Brooks said "Feel good about the fact that in the bivalent we saw no signal from myocarditis," he said after the presentation. "Very important." Dr. Brooks, chief medical officer at Watts Healthcare Corporation, did not respond to an inquiry.”
Hmm. VSD is a smaller safety system than VAERS, ran for only half the period for which VAERS data was available and Dr Brookes has a “feel good” sensation because there was no signal on VSD.
No mention of VAERS or any need to adjust for KNOWN under-reporting of “events”.
At which point (and with a sigh) I thought I would go over what is happening in the area in the real – non-CDC clown – world, just to put the bivalent safety issue in some sort of context.
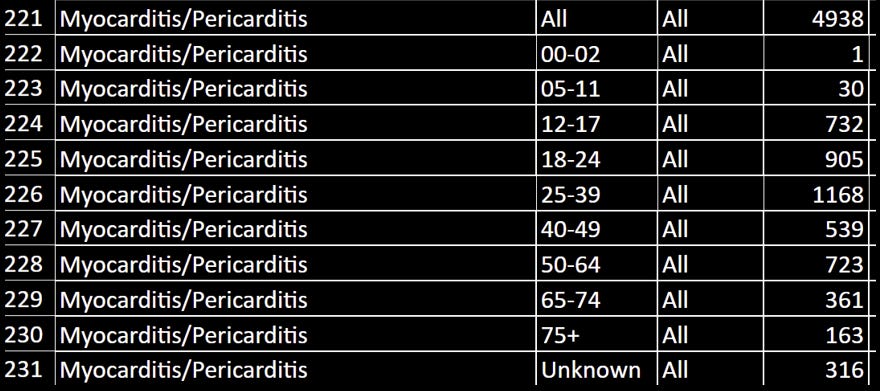
All time myocarditis from here:
CDC VAERS Safety Signals Summary for COVID-19 Vaccines through 9/15/2023 – VAERS Analysis
And this:

I am not sure if the latter table is a subset of the former.
The experimental bivalent doses were emergency use authorized on 21 August 2022.
Around 22 million doses of all types were administered in the US over the seven weeks post 21 August 2022. Probably 20 million would have been the bivalent doses. So the 98 cases extracted by the Epoch Times from VAERS would represent around 5 per million cases or a tiny 0.0005%
I have seen far higher numbers referenced in studies around the world, somewhere between 3% and 5% - the numbers above are for cases, not deaths.
It’s not just the CDC that is woefully out of date and using stale information. I spotted this from the UK government:
“In a pre-COVID-19 study from the UK it was estimated that between 1998 and 2017 there were 36.5 per 100,000 NHS admissions with myocarditis..” So perhaps that is a base, starting position…”
It has this to say about myocarditis caused by SARS-COV2 infection.
“It is now recognised that COVID-19 infection can lead to myocarditis or pericarditis and in one retrospective study, 5% of patients developed new onset myocarditis and 1.5% pericarditis within a 6 month period following COVID-19 infection .”
It references the Israeli study, but presents figures that imply that myocarditis from infection dwarfs myocarditis from injection.
“n one of the largest studies published to date on the Israeli experience, over 2 million individuals were assessed. The estimated incidence of myocarditis was 2 per 100,000 individuals, with the highest reported rate in males aged 16 to 29.”
2 per 100k = 20 per million v 50,000 per million from the infection.
It seems that the UK government wishes to convey an alternate reality.
Compare that to this: from January 2023
And this:
13 million Americans with myocarditis from 677 million doses. For ease, lets say 250 million Americans have been dosed twice. The rate of myocarditis becomes 52,000 per million – 5.2%.
Does this help solve the issue of the relative risks of myocarditis from the old bivalent and the very old monovalent shots – or allow a baseline for the new monovalent shot? Well, no, not really! But the data is there somewhere, even though it will still have to be adjusted for under-reporting!
One can’t help but wonder if myocarditis is just one of a dozen potentially lethal harms that just happens to be most visible. Other harms causing deaths are being ignored or swept under the carpet or perhaps simply attributed as normal causes of deaths – but whose rates of death far exceed historical norms – like turbo cancers, diabetes, liver disease, or even Alzheimer’s that might actually be “brain fog” caused by mRNA injections where the spike protein has penetrated the blood brain barrier.
Is there a brain expert who has the equivalent expertise that Dr McCullough has in hearts?
Whew.. I need a coffee!
Onwards!
Please buy a subscription or donate a coffee (I drink a lot of coffee) - “God Bless You!” if you can’t or don’t want to contribute. Coffee donations here: https://ko-fi.com/peterhalligan - an annual subscription of 100 bucks is one third less than a $3 coffee a week!
Peter Halligan, You are the Best!
I know more than 30 people killed by this murder shot