

The false pandemic and the pandemic of the vaccinated - four phases of "C19"

First a reprise of the first three phases.
Phase 1 – Outbreak, Phase 2 – Injection Roll-out, Phase 3 – Outturn
We know that the RT-PCR test was designed to detect the presence of sequences, not infectiousness. We know that the number of false positives is around 90-95% once the number of amplification cycles used exceeds 30. We know that the average age of those “diagnosed” using the RT-PCR test exceeds average life expectancy by a year or two and that those that succumbed had somewhere between 2 and 6 co-morbidities.
We now know from here that deaths with C19 present were clustered amongst the poor and the sick (though we need to do more analysis on race and gender) and that excess deaths are NOT correlated with age.
Notwithstanding all that, it is worth looking at what the “official” position is – to see what the propaganda is telling us.
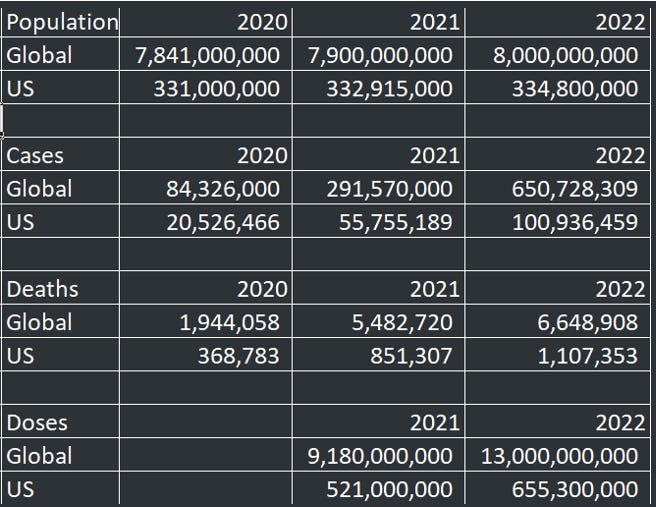
Using data for US cases and deaths, Global Cases and Deaths and combining this with US injections and Global injections and then converting the data into numbers per million (adjusting to reflect only those globally that have received at least one dose, we have this table.
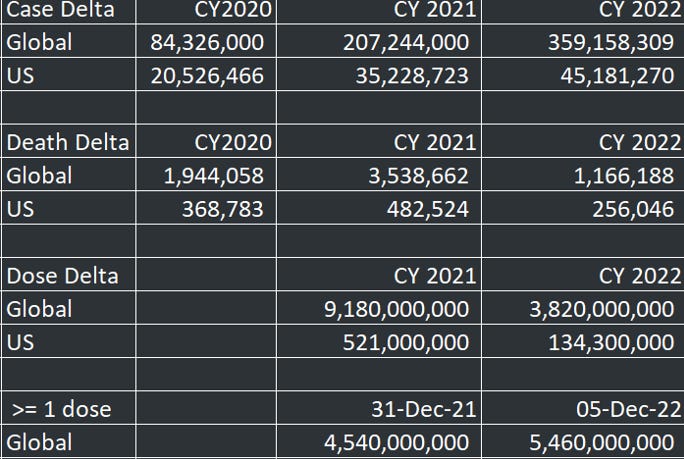
These numbers are the changes within each calendar year that correspond to three phases: 2020 – C19 only, 2021 – increasing injection roll-out, 2022 so far – largely a completed initial course.

From that table, the number of “cases” misdiagnosed using the RT-PCR and RAT testing method have increased markedly but the rate of deaths with C19 “present” per case have dropped a lot. Remember that around 10% of the US was diagnosed as a “case” between December 2021 and February 2022 (circa 35 million “cases”).
Those not interested in the underlying data can skip the next tables.
Okay, that’s the “official” view.
Perhaps we can take solace from the substantial decline in the rate of injections over 2022, compared to 2021.
Now for some conspiratorial truth bombs.
First – around only around 5% of those that died with C19 “present” as diagnosed by the RT-PCR/RAT tests, died from C19. Ninety-five per cent of people died from
· the failure to treat with anti-biotics or continue treatment
· failure to continue treatment for existing conditions
· failure to diagnose new, life threatening conditions
· psychological stress from “non-pharmaceutical interventions” (NPI’s) – e.g neglect and forced isolation/house arrest/deprivation of family support/eradication of self-worth
· treatment protocols involving Remdesivir, respirators, denial of vitamins/food/water in hospital settings, stipulated by the likes of Fauci, Collins and Birx.
All these deaths were preventable with treatment protocols or removal of NPI’s, but the measures enforced by the FDA/CDC/NIH/NIAID cabal and the WHO, were directly responsible.
Hopefully, a fall in the number of deaths coincides with better treatment over 2022.
Rather than a test of whether C19 was present, autopsies must be performed on those that died (and who were not cremated) to determine the prevalence of Remdesivir (or Midazolam plus morphine for the UK) AND prevalence of spike protein correlated with C19 or vaxx spike proteins.
In previous articles, I showed the tables for leading causes of death and the ages of those that died over the first two phases – 2020 and 2021.

(Note that drug overdoses numbering around 140,000 or so did not make this list, extracted from the CDC web site.)
This conspiracy theory/hypothesis contends that around 40,000 of 766,000 deaths with C19 present were actually from C19 (the new ‘flu). The rest should be allocated across (mostly leading) other causes of death
Here is the two year change in death by age cohort:

We can only wait and watch for the 2022 numbers; I stopped reading this at page 20 of 36.
Secondly, we have discovered that the “vaccine” approval process is so badly flawed that the entire “vaccine” schedule needs to be revisited. We know that the question of deaths and injuries reported to VAERS is substantially understated. We now know that the “vaccine” approval process employed by the FDA/CDC does NOT monitor adverse events over time and that “placebos” used in most “vaccines” are NOT placebos at all, they compare a new “vaccine” with an old “vaccine”. (There are still “vaccines” on the child schedules that contain mercury and aluminium).
The ”vaccine” schedule needs an overhaul (enema) to correlate developing trends in health and death with previous “vaccine” roll-outs over the last five decades (of Fauci’s reign) to restore public trust and public health.
Thirdly, we can estimate the butchers bill of the roll-out of C19 injections – mRNA and viral vector injections. The correlation between excess mortality and its correlation with C19 injections must be completed for each dose and demographic. Of note, Florida Surgeon General Ladapo found no excess mortality overall in Florida, whilst finding excess deaths amongst young men. There is useful information to be had about gender specific efficacy that differentiates suitability by gender. By implication, women receive a benefit If there is no overall excess mortality.
Which brings us to the Fourth Phase – treatment of the vaxx damaged and accurate diagnosis of emerging C19 cases.
Suffice to say, in a worst case scenario, one fifth of the population has already suffered symptomatic adverse events that provide a warning of potential morbid conditions. We need to be able to test for vaxx damage with the same intensity and frequency as we test for C19. We need solutions to the presence of the toxic spike protein In the blood and organs. It goes without saying that the injection roll-out has to be terminated immediately.
Perhaps the people in big pharma can turn their attention to solving this problem instead of creating it.
Maybe the wizards of CRISPr could develop a solution (if they haven’t already). Maybe we can enhance the miracle drug IVM by giving some sort of POSITIVE gain of function.
Perhaps we can program some nanobots to go into the bloodstream (with clear proof of success and extraction of nanobots once complete!) and “search and destroy” the spike proteins – or do some work around an electro-magnetic pulse or 5G signal that destroys or allows “concentration for extraction” of the spike protein.
I personally would need decades of training before I could even attempt a solution – others already have that training. We need a task force to develop solutions in the same way that a C19 task force exists.
In the meanwhile, hospitals need to be re-tooled with the necessary equipment to diagnose and treat as best they can, the massive numbers of incoming vaxx damaged people.
Excellent, excellent piece Peter- thank you.
Problem-Reaction-Solution- a time honored strategy.
Without the fear-mongering propaganda campaign no one would’ve noticed anything unusual about the last two flu seasons because there was nothing unusual, except for the criminal, murderous, and utterly unscientific lockdown policies and "health protocols" in response to the non- existent threat.
"Covid-19" deaths follow the same age/risk stratification and seasonal curve of flu/pneumonia at the same time that flu inexplicably vanished from the face of the earth while all pneumonia deaths were suddenly called “Covid” using mass death certification fraud.
I cut my teeth on the massive amount of corruption and profiteering and Pharma con jobs back in 2005 with the Avian Flu hoax. They tried the same con, with mostly the same cast of characters, in 2009/10 with the Swine Flu hoax.
I spent a lot of time in both instances trying to alert people throughout the community to the realities of these frauds. Each time there was tremendous push back followed by acknowledgement that these were indeed scams. However it seems that there is a bizarre psychotic thirst for this hysteria in our present culture as after each fraud was proven it only needed a few years passing for these very same folks to become ready to accept a new fraud.
Once you have explored the details of these frauds it is easy to identify the scam as it is happening.
The playbook is pretty much the same, they simply refine the techniques. Not so easy to convince others of the scam as they are bombarded with fear porn 24/7.
I have to say that the "messaging" is far more comprehensive, insidious and sophisticated with Operation Covidius than all others before by quantum leaps.
That and they produced the cadavers this time through an array of medical democides (remdesivir, neglect, midazolam, ventilators, etc.) which solidified the fear mechanisms in the masses.
It's breathtaking really to witness the grip of fear this had and still has on millions and a vast number of these people will be damaged for life. The shadow of this psychosis will follow them to their graves. This is particularly true among the "educated" classes who now have a warped sense of purpose beyond the dull, aimless wanderings of Academia.
As for the Covid™ fable of 2020 itself, it was and is a nasty lie- all of it from top to bottom. All of the exaggerated and repeated fear-based messages from the media and government agencies this past two and a half years were just part of the advertising campaign for the pharmaceutical industry’s newest lucrative product- the mRNA vaccine cash cow-which they hope to roll out as a new medical delivery system for a variety of chronic “ailments”, e.g. new line of “cancer vaccines.”
Every single one of the media bullhorns that were blasting the Covid fiction for the past two plus years have direct financial ties to Pharma Inc. It’s not exactly accurate to say Pharma uses its power to influence the news- more to the point it is Pharma that writes the script. Pharma and it’s investors own “the news” and you will speak the Pharma gospel if you wish to maintain your position of privilege as a Pharma propagandist- it goes without saying.
When we speak about Pharma this cannot be separated out from the investor class who rakes in oceans of taxpayer wealth through numerous Pandemic Ponzi Schemes with Pharma as it’s “sacrificial offering” and its Trojan Horse.
"Covid-19" is a business plan not a medical emergency. Now more than ever it’s important to understand the economics of vaccines. Traditional systems of vaccine procurement and distribution are rapidly giving way to vast public–private supply chains. Despite annual revenues over $1 trillion, the industry has been unable to reverse a declining rate of profit and finds itself in a perpetual state of crisis.
In Fall/Winter of 2019 all stocks of Big Pharma companies were in steep decline. This changed dramatically in Spring 2020 as we now know. The experimental gene therapy mRNA drugs are set to become the most lucrative drugs in medical history. Pharma depends on its “blockbuster drugs” to remain profitable and appealing to investors. It is not an exaggeration to say that without these “blockbuster drugs” the Pharma industry implodes.
What happened in 2020 was simply that the flu was re-branded and repurposed- the term "Covid-19" was invented to turn the seasonal virus into the equivalent of the mythical “Al-Qaeda” to terrorize the population with yet another media constructed boogeyman.
This was done as the Western economies were in total free fall in late 2019 and the plan to digitize the economies of The West had to be rushed through lest the collapse be seen for what it was- the by-product of decades of Ponzi schemes by the Wall St. parasites and their allies.
The Virus™ is superfluous, just like the Swine Flu scamdemic of 2009. All they needed to do was create the perception of a pandemic/mass panic with staged Hollywood productions, doomsday models, and the fraudulent PCR test to manufacture the cases/falsely attributed as “Covid deaths.”
Yes - thank you - for saying it. It time to dispense with the BS and move forward toward helping the vaccinated. Whatever happened to get us to this point doesn’t matter anymore. The only thing that matters now is keeping as many as we can from dying from this poison.